Program Progress:
Click the play button to complete this section. To view any topic, select the button below.
Apex video
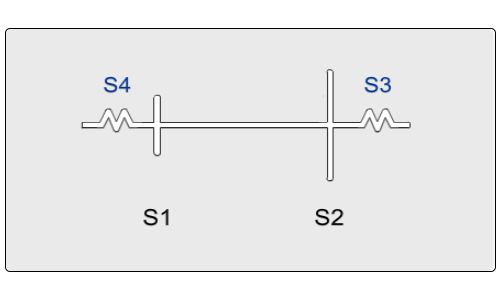
Let us evaluate together the acoustic events at the apex. We shall use the cotton swab on the carotid vessel, so that we can recognize systole and we should use the bell of the stethoscope at the apex. Let us listen together. [Cut-away]What did we hear at the apex? Well, the most compelling thing we heard were the low frequency sounds. There was an S4 and an S3. We didn't just hear [sound], but we heard [sounds]. The fourth sound just before the first sound and the third sound just after the second sound. There was also a subtle observation, when we listened, the first sound, that should normally be louder than the second at the apex, was actually a bit softer. That is, we heard a diminished first heart sound. Now, in the clinical setting with acute infarction, that could be possibly due to a prolonged PR interval, but it also may be due to a reduced ventricular contractility. But, let's go back to the best reflectors of reduced ventricular contractility, and that is the filling sounds. Again, we heard [sounds]. Now, the fourth sound that precedes the first sound is so very common in the setting of acute myocardial infarction, that it is heard in many cases where it's a very mild degree of muscle damage or ischemia. But the third heart sound is clearly a significant reflector of ventricular failure, a reduced compliance of the ventricle, of ventricular ischemia. So that was the key finding we heard at the apex. Sometimes, when the heart rate becomes more accelerated, these filling sounds can fuse together, it's almost like a cantering horse, or a gallop sound, that's been called a summation gallop, where you will hear [sounds]. But, in our case, again, [sounds].
Oscilloscope
By viewing an oscilloscopic image and simultaneously listening, we can further appreciate these auscultatory events.Review Apex Tracing